Download PDF: Pharmacology of Prokinetic Drugs and Antiemetics
Acquire detailed PDF notes or potential PPT slides that thoroughly cover Prokinetic Drugs and Antiemetics. This resource delves into their pharmacology, including diverse mechanisms of action, key classifications, clinical indications for GI motility disorders (like gastroparesis) and the management of nausea and vomiting from various causes, and important side effects. Essential for students of medicine and pharmacy. Download your free prokinetics and antiemetics PDF or view it online.
Keywords: prokinetic drugs pdf download, antiemetics pharmacology notes, GI motility drugs ppt, metoclopramide mechanism, ondansetron uses, treatment of nausea and vomiting, gastroparesis drugs pdf, free medical notes download, view online pharmacology.
Pharmacological Insights into Prokinetic and Antiemetic Agents
Prokinetic and antiemetic drugs are vital therapeutic classes for managing a spectrum of gastrointestinal (GI) motility disorders and the distressing symptoms of nausea and vomiting. Prokinetics aim to enhance and coordinate GI transit, while antiemetics target the complex pathways of the vomiting reflex. A clear understanding of their pharmacology is crucial for their effective and safe clinical application.
Prokinetic Drugs: Enhancing Gastrointestinal Motility
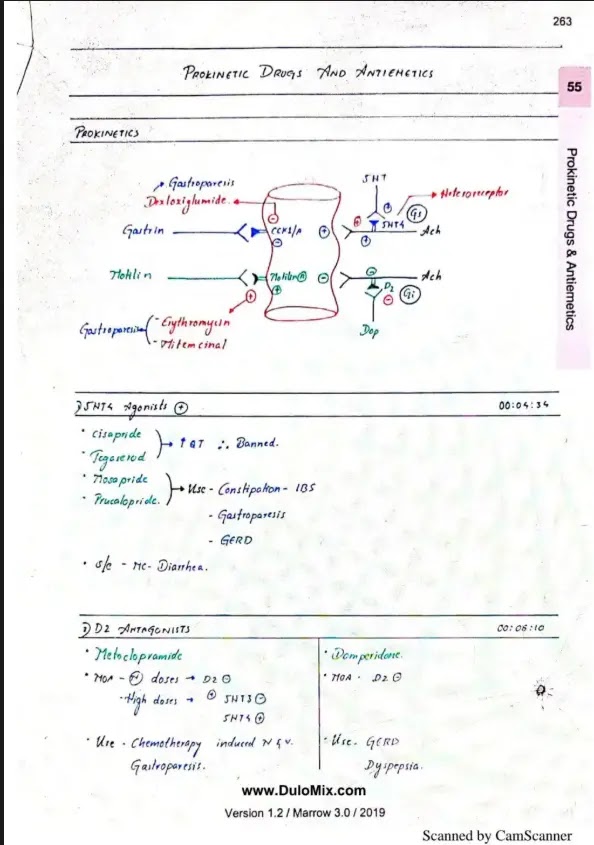
Prokinetic agents are defined by their ability to stimulate coordinated contractions that propel contents through the GI tract. They are primarily used in conditions like gastroparesis (delayed gastric emptying), gastroesophageal reflux disease (GERD) by increasing lower esophageal sphincter (LES) tone and esophageal clearance, and some forms of functional dyspepsia or chronic constipation.
Key Mechanisms and Drug Classes:
-
Dopamine D2 Receptor Antagonists:
Dopamine acts as an inhibitory neurotransmitter in the GI tract via D2 receptors. Antagonizing these receptors disinhibits cholinergic neurons, leading to increased acetylcholine release, which enhances motility.
- Metoclopramide: Centrally and peripherally acting. Increases LES pressure, accelerates gastric emptying, and enhances small intestinal transit. Also possesses antiemetic effects by blocking D2 receptors in the chemoreceptor trigger zone (CTZ). Crosses the blood-brain barrier, potentially causing extrapyramidal symptoms (EPS) like dystonia, akathisia, parkinsonism, and tardive dyskinesia, especially with long-term use or in vulnerable populations.
- Domperidone: Predominantly a peripheral D2 antagonist due to limited CNS penetration, resulting in fewer EPS. However, it carries a risk of cardiac arrhythmias (QT prolongation and ventricular arrhythmias), leading to restrictions on its use.
-
Serotonin 5-HT4 Receptor Agonists:
Activation of 5-HT4 receptors on enteric neurons stimulates acetylcholine release from myenteric motor neurons, promoting peristalsis.
- Prucalopride: A selective, high-affinity 5-HT4 agonist approved for chronic idiopathic constipation in adults when laxatives fail.
- Historical agents: Cisapride (withdrawn due to cardiac toxicity) and Tegaserod (restricted use due to cardiovascular concerns) also acted via this mechanism.
-
Motilin Receptor Agonists (Motilides):
Motilin is an endogenous peptide that stimulates GI motility, particularly in the upper GI tract, during the interdigestive phase.
- Erythromycin (Macrolide Antibiotic): At sub-antimicrobial doses, erythromycin acts as a motilin agonist, potently stimulating gastric emptying. Its utility is limited by rapid development of tachyphylaxis (tolerance) and concerns about antibiotic resistance and drug interactions (CYP3A4 inhibition).
-
Ghrelin Receptor Agonists:
Ghrelin, the "hunger hormone," also has prokinetic effects. Agonists are being investigated for gastroparesis.
-
Acetylcholinesterase Inhibitors (e.g., Neostigmine):
By increasing acetylcholine availability, these can stimulate colonic motility and are sometimes used for acute colonic pseudo-obstruction (Ogilvie's syndrome).
Antiemetic Drugs: Combating Nausea and Vomiting
Antiemetics are a diverse group of drugs that prevent or alleviate nausea and vomiting. The vomiting reflex is a complex process coordinated by the vomiting center in the medulla, which receives inputs from the CTZ, vestibular system, higher cortical centers, and visceral afferents from the GI tract. Different antiemetics target various neurotransmitter receptors involved in these pathways.
Key Mechanisms and Drug Classes:
-
Serotonin 5-HT3 Receptor Antagonists ("Setrons"):
Block 5-HT3 receptors on vagal afferents in the GI tract and in the CTZ and vomiting center. Highly effective for chemotherapy-induced nausea and vomiting (CINV), radiation-induced N/V, and postoperative nausea and vomiting (PONV).
- Examples: Ondansetron, Granisetron, Dolasetron, Palonosetron (longer half-life, higher affinity).
Side effects: Headache, constipation, dizziness; rare QT prolongation.
-
Dopamine D2 Receptor Antagonists:
Block D2 receptors in the CTZ. Effective for various types of N/V.
- Phenothiazines (e.g., Prochlorperazine, Promethazine - also H1 antagonist/anticholinergic).
- Butyrophenones (e.g., Haloperidol, Droperidol - droperidol has black box warning for QT prolongation).
- Metoclopramide and Domperidone (as above).
-
Neurokinin-1 (NK1) Receptor Antagonists:
Block the binding of substance P to NK1 receptors in the CTZ and vomiting center. Particularly effective against delayed CINV and often used in combination with 5-HT3 antagonists and corticosteroids.
- Examples: Aprepitant (oral), Fosaprepitant (IV prodrug), Rolapitant, Netupitant (often co-formulated with palonosetron).
-
Antihistamines (H1 Receptor Blockers):
Primarily effective for motion sickness and vestibular disorders by acting on H1 receptors in the vestibular nuclei and brainstem. Many also have anticholinergic properties.
- Examples: Cyclizine, Meclizine, Diphenhydramine, Dimenhydrinate, Promethazine.
Side effect: Sedation is common.
-
Anticholinergics (Muscarinic Receptor Antagonists):
Block muscarinic receptors in the vestibular system and vomiting center. Most effective for motion sickness.
- Example: Scopolamine (Hyoscine), often used as a transdermal patch.
Side effects: Dry mouth, drowsiness, blurred vision.
-
Corticosteroids:
Mechanism not fully elucidated but thought to involve prostaglandin inhibition and effects on serotonin pathways or blood-brain barrier permeability. Used as adjuncts, especially for CINV and PONV.
- Example: Dexamethasone.
-
Cannabinoids:
Agonists at CB1 receptors in the CNS. Used for refractory CINV and as appetite stimulants.
- Examples: Dronabinol, Nabilone.
-
Benzodiazepines (e.g., Lorazepam):
Primarily for anticipatory N/V associated with chemotherapy, due to anxiolytic, sedative, and amnesic effects.
The selection of prokinetic or antiemetic therapy is individualized based on the underlying cause, severity of symptoms, patient characteristics, and the specific pharmacological profile of the chosen agent, including its efficacy and potential adverse effects. Combination therapy is often employed in managing severe emesis, particularly CINV.
Info!
If you are the copyright owner of this document and want to report it, please visit the copyright infringement notice page to submit a report.